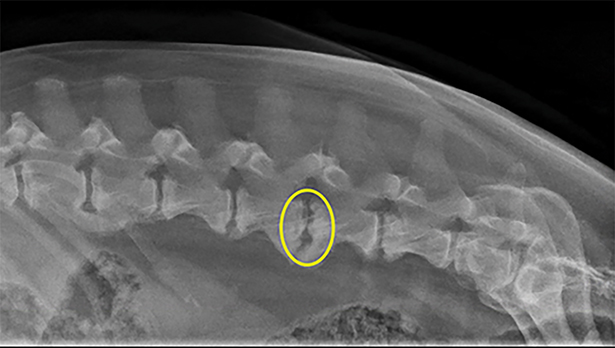
Above: Spinal radiographs from a dog with discospondylitis at L4-L5 (yellow circle). Note the lysis of the vertebral endplates.
We have all had patients that we would love to refer to a specialist but for whom, unfortunately, this option was not feasible. There are still options to provide your patients and clients for medically managing patients with myelopathic disease. When determining a treatment plan for patients with myelopathies, it is crucial to consider the most appropriate differentials for that specific patient.
The patient’s signalment, history, and examination findings can provide information to assist with prioritizing your differentials. In older patients, degenerative (intervertebral disk disease [IVDD], degenerative myelopathy), neoplastic, vascular, and inflammatory conditions are going to be more likely. In younger patients, inflammatory/infectious conditions, congenital anomalies (<6 months), and degenerative (IVDD) diseases are also considered. Remember that IVDD is often not seen in dogs (even dachshunds!) until at least 2 years of age. The breed of dog may also assist with formulating your differential list.
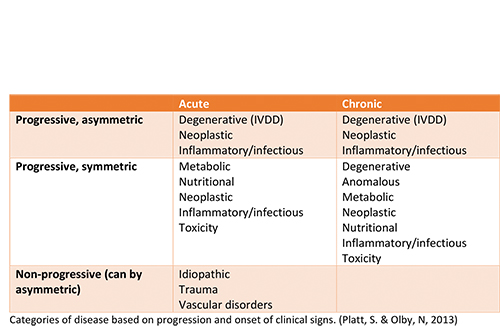
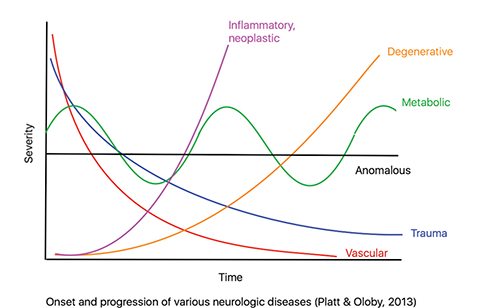 From the history, we can determine if the signs are acute versus chronic, the progression of clinical signs, and if the onset of signs were associated with any injury or event. Certain disease processes, such as Type I IVDD, vascular (fibrocartilaginous embolism, FCE), trauma (fracture/luxation or acute noncompressive nucleus pulposus extrusion [ANNPE]), or inflammatory (infectious or immune mediated) typically have a very acute onset of clinical signs. Other conditions, such as Type II IVDD, neoplasia, degenerative myelopathy (DM), and congenital anomalies may have a more chronic history.
From the history, we can determine if the signs are acute versus chronic, the progression of clinical signs, and if the onset of signs were associated with any injury or event. Certain disease processes, such as Type I IVDD, vascular (fibrocartilaginous embolism, FCE), trauma (fracture/luxation or acute noncompressive nucleus pulposus extrusion [ANNPE]), or inflammatory (infectious or immune mediated) typically have a very acute onset of clinical signs. Other conditions, such as Type II IVDD, neoplasia, degenerative myelopathy (DM), and congenital anomalies may have a more chronic history.
The progression of clinical signs and the findings of the physical and neurologic examination are also useful. In patients that are febrile, an inflammatory process should be considered. There are also certain diseases that affect specific regions of the spinal cord. For example, cervical spondylomyelopathy (CSM) affects the cervical spinal cord whereas patients with degenerative myelopathy present with signs of a thoracolumbar myelopathy.
Lastly, does the patient have spinal hyperpathia on examination? Painful conditions include IVDD, inflammatory/infectious disease, trauma, and neoplasia. Diseases considered to be non-painful include degenerative myelopathy, FCE, ANNPE (after first 24 hours), and metabolic disorders.
On the basis of your differential diagnosis list, you can make diagnostic testing recommendations. Routine bloodwork and urinalysis are recommended to rule out underlying metabolic conditions. Spinal radiographs are of benefit in regard to ruling out potential osteolytic lesions due to neoplastic or infectious process, such as discospondylitis. Remember that radiographic changes may not correlate to the severity of clinical signs. Testing for infectious disease, including Toxoplasma, Neospora, tick-borne disease (Tick PCR), and potentially fungal disease, is also recommended.
Treatment can be based around what are considered the most likely causes. Pending results of infectious disease testing +/- culture, or if infectious disease is highly likely, empiric antimicrobial therapy can be initiated. If the patient shows signs of spinal hyperpathia, pain-relieving medication options include gabapentin and amantadine. The use of an anti-inflammatory medication is also reasonable.
When choosing between a corticosteroid and an NSAID, some things to consider include the most likely disease process and patient comorbidities. An NSAID will not treat autoimmune disease, and the patient may require a washout period if switching to a corticosteroid is indicated. Corticosteroid use could worsen the clinical signs in a patient with infectious disease and, in recumbent patients, may increase the risk of UTIs, pressure sores, and urine scald. If there is any potential for a referral, steroids may also make a diagnosis difficult in the case of inflammatory autoimmune diseases or lymphoma. Therefore, NSAIDs are preferred in many cases unless there is a strong suspicion for inflammatory disease.
Remember that if the underlying cause is unknown, activity restriction is recommended for at least 4 to 6 weeks. Rechecking patients to assess their neurologic status and their response to treatment is important so that further recommendations and/or medication adjustments can be made.
In summary, when presented with a patient suffering from myelopathic disease when referral is not possible, prioritize your differential diagnoses based on the signalment, history, onset/progression, and examination findings to help guide you with further diagnostic testing and treatment options.
VTHNeurology@vetmed.illinois.edu
By Kari Foss, DVM, MS, DACVIM (Neurology)


