This case summary was written by Ellie Andersen, a second year veterinary student volunteer, as part of our student blog series.
History: A red-tailed hawk was brought in to the clinic on November 22nd. It was found on the ground in front of a barn, and did not resist capture or attempt to fly away.
Physical Exam: On physical exam, triage volunteers found that the hawk was very emaciated with a body score of 1 out of 5. Several hippoboscus flies were found on the patient, and the back of the bird’s throat was pale with a corrugated appearance. The patient also had a few strings in the mouth, and was estimated to be 6% dehydrated. An old ulnar fracture was palpated on the right wing, and it felt calloused and stable. No other abnormalities were found. The primary problem appeared to be emaciation at this time.
Initial Treatments: The initial treatments for this patient were performed during the week of Thanksgiving, while most students went home, and a few volunteers remained to run the clinic. The patient was started on fluid therapy and received SQ (subcutaneous) LRS (fluids) in the inguinal flaps for 3 days. The patient was also gavage-fed carnivore care at a 3:1 dilution at intake, and was weaned up to the full concentration over a few days. Next, volunteers began offering the hawk skinned mice in the cage. The patient began eating on its own within a few days.
Bloodwork: A Packed-Cell Volume test was performed, and the blood cell concentration was found to be 19%. Volunteers and veterinarians decided that the low PCV was probably due to emaciation. We wanted to make sure that there wasn’t an underlying disease causing the emaciation, so a blood smear test and Complete Blood Count (CBC) were performed. The white blood cell count on the smear appeared to be within normal limits. There were no significant findings on the CBC results.
Radiographs: Our team needed to get radiographs on the right wing to make sure the
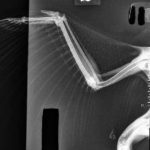
old fracture wasn’t preventing this patient from flying. We also wanted to get systemic (full body) radiographs in preparation for this patient’s transfer to the Illinois Raptor Center (IRC), and eventual release back to the wild. The old fracture on the ulna appeared to have formed boney callous around it, indicating appropriate healing progression. The systemic images showed no abnormalities.
Patient Care and Transfer: My involvement with this case was mainly helping with patient care. I assisted with feeding the patient and giving medications. We began by maintaining the patient on a diet of thawed mice and cut-up chicks. We added Itraconazole PO (orally) to our nightly treatments to prevent an aspergillosis infection, because we knew the patient would be in the clinic for a few weeks while he gained weight. The patient gained weight quickly and was consistently BAR (bright, alert, and responsive) and evading capture. As the patient gained weight, we increased the amount of food he was getting to 120 grams a day. The patient began to run up to the front of the cage when food was being offered. Over three weeks, the patient gained 160 grams and reached a healthy body condition score. With the clean results from the blood work and radiographs, our team felt confident in transferring (and eventually releasing) this patient. I captured and boxed the patient up on the morning of December 5th, and he was transferred to IRC for flight rehabilitation.