
Fracture Planning:
Developing an appropriate plan involves the following sight interrelated steps.
Follow along the steps with the sample case in the right column or download and print the sample case.
Fracture Planning:
Developing an appropriate plan involves the following interrelated steps.
(open the sample case.pdf to review as you go through this section)
Radiographs are made of the fractured bone (and frequently of the contra lateral bone to serve as a template for restoring limb alignment and bone length and as a guide to fixation size and contour). Fractures are classified according to the location of the fracture, (right or left, bone, location within the bone (diaphyseal, metaphyseal physeal, articular) and the direction and number of fracture lines. Along with learning to describe a fracture accurately to a specialist, much of the description gives you clues about the fracture to use in decision making and planning.
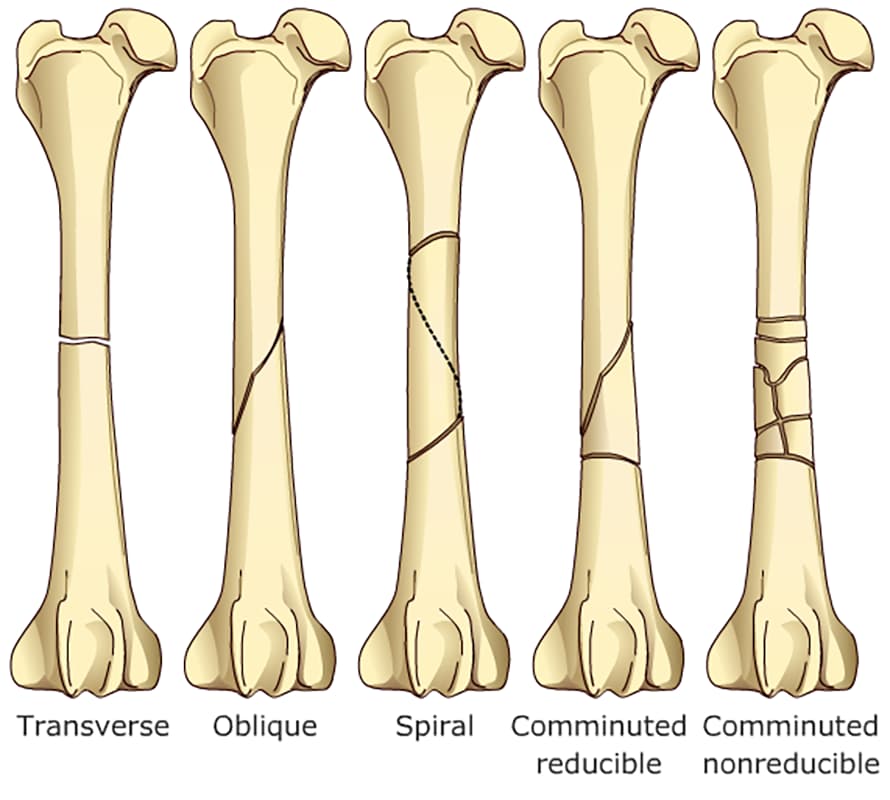
Transverse: perpendicular to the long axis of the bone
Oblique: runs at an angle to the long axis of the bone
- Short oblique = ≤ 45 degrees to the long axis
- Long oblique = ≥ 45 degrees to the long axis
– Spiral: wrap around the bone
– Comminuted: multiple fracture lines ( at least 3 pieces)
* Butterfly fragment = 2 oblique fracture lines with a large cortical fragment; (it is usually reducible)
*Highly comminuted = multiple pieces resembling a “shattered” appearance; ( usually non-reducible)
The displacement of the fracture on the current radiograph, the apparent reducibility of the fracture; and whether it is open to the environment.are all important descriptors
2-5 Come up with a fracture assessment score to guide your decision making for optimal treatment
After the patient has been thoroughly examined and life-threatening problems corrected, fracture treatment planning is performed. This includes assessing preoperative patient data such as age, weight, general health, activity level, and presence of other orthopedic pathology or neurologic pathology. Radiographs of the fractured and corresponding contralateral intact bones, which including the joints proximal and distal to the fracture; are closely examined as additional information can often be gathered (open physes are a dead giveaway that the patient is immature and biologically a healing machine and gas patterns at the fracture strongly suggest an open fracture. Client information such as their expectations and ability to perform postoperative care are also important to consider as you choose your fixation.
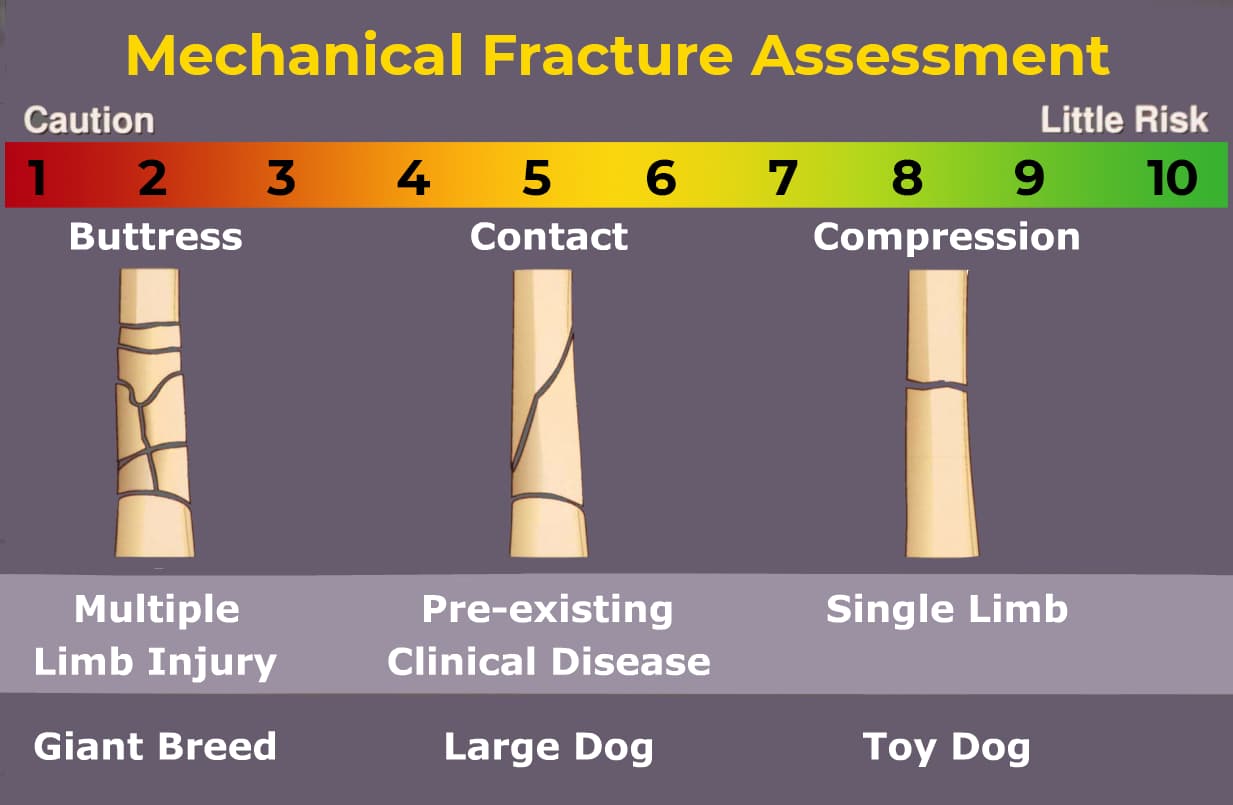
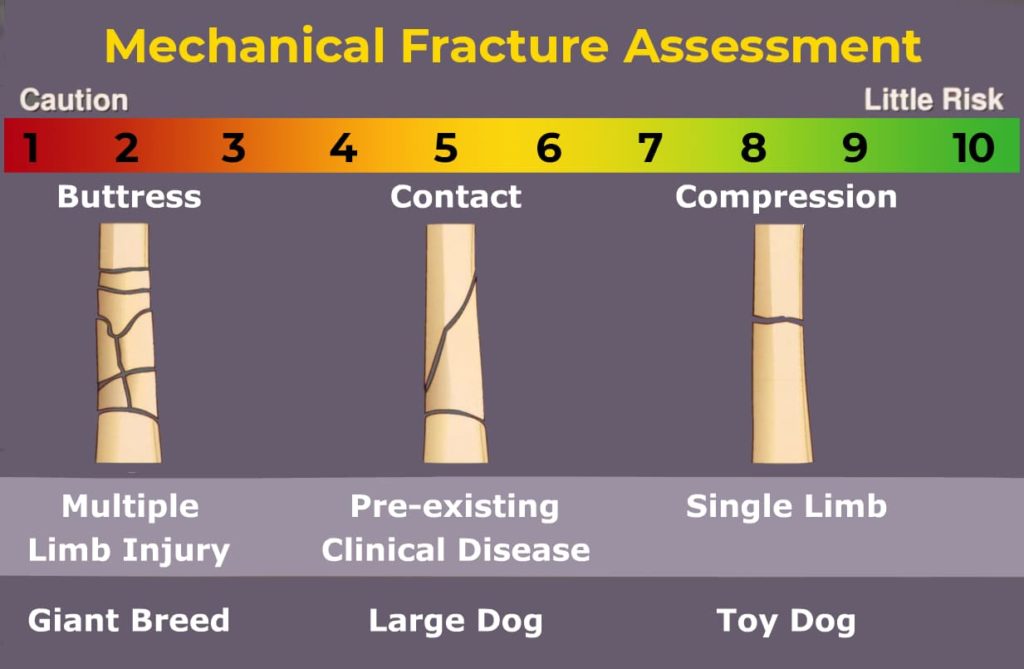
The mechanical score indicates how strong the implant must be.
A restored bone column which can transfer weight bearing load will help protect the implant from fatigue. Conversely an unreconstructed fracture depends on the implant to sustain the load of weight bearing. An animal with additional limb injuries or pre-existing pathology will be less able to protect the fractured limb and implant.
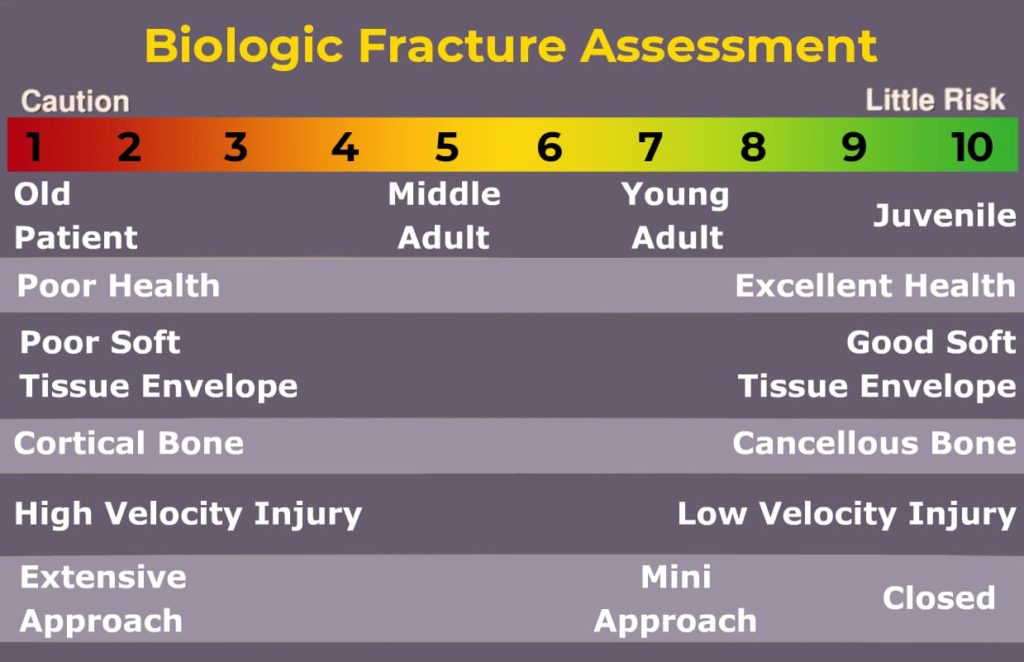
The Biological score indicates how long implant must function.
An immature animal with an active periosteum will heal very quickly. Conversely, an older or otherwise compromised animal will require a longer healing period. Fractures through the cancellous bone of the metaphysis will heal more quickly than diaphyseal fractures. Fractures with severely interrupted vascularity and disturbed surrounding soft tissues will require a longer healing period. Implants subjected to slow healing conditions must be larger, stronger and able to remain in position for extended periods to minimize chances for cyclic fatigue of the implant. Comminuted fractures with disturbed vascularity are best treated with biological techniques of major segment alignment and bridging osteosynthesis.
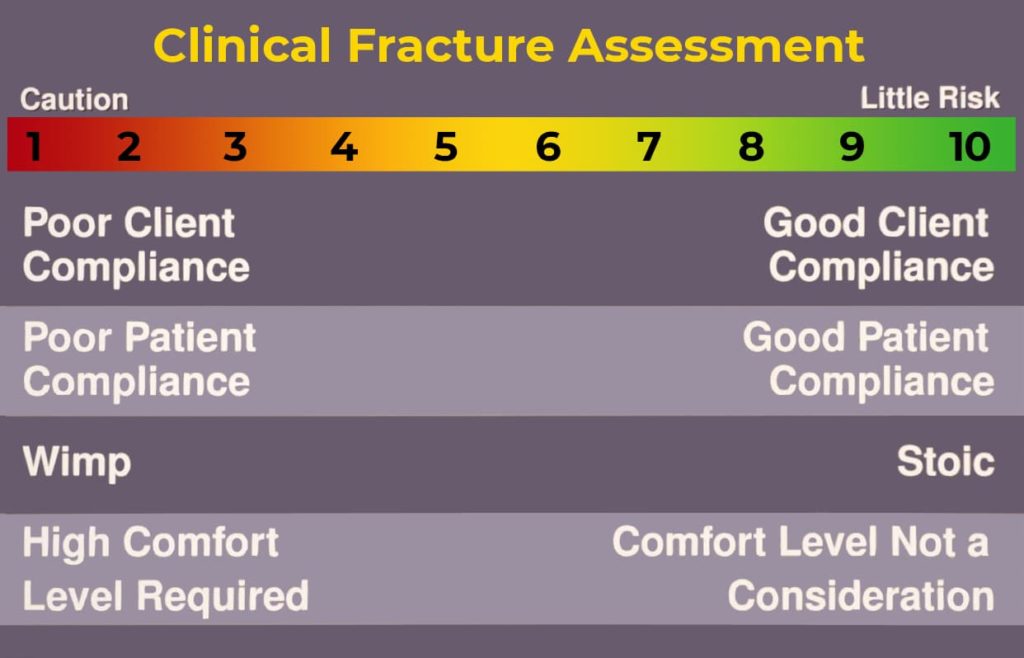
The clinical score indicates the level of postoperative care the owners can provide.
A co-operative animal with an attentive owner willing to follow directions is an asset. Active animals allowed excessive exercise must be treated with larger, stronger implants.
Come up with a FAS score from 1 to 10 by combining mechanical biological and clinical scores (see sample case for application of mechanical, biological and clinical assessment of the fracture and patient). Fractures with anticipated slow healing NEED functional implants for a long time. Implants subjected to unfavorable mechanical environments must be larger, stronger and remain in position for extended periods. An example would be adding ancillary fixation like an intramedullary pin (pin/plate combination), choosing a larger plate with more screws, or selecting an interlocking nail.
- 1-3 FAS tells you to use a very strong fixation and lots of biological as this animal may be a slow healer with inattentive owners
- A high middle score usually indicates an animal with a reconstructable fracture but unfavorable biology
- A low middle score may reflect a young dog with a severely comminuted fractur e which is nonreducible
- score of 8-10 indicates a healing machine with a reconstructable fracture and very attentive owners
Reduction of the fracture is the act of either making the bone fit together or aligning the joints depending on the animal and the fracture. Reduction may be accomplished in a closed fashion (not exposing the fracture) or open (making a surgical approach to the fracture) the fracture reduction animations illustrate these actions.
Decide whether to perform an open or closed reduction by the following indications.
Review reduction videos
Open Reduction
- Articular Fractures
- Anatomically reconstructable fractures
- Comminuted fractures treated by major segment alignment and cancellous bone graft
Closed Reduction
- Nondisplaced or incomplete fractures
- Comminuted fractures treated by major segment alignment using bridging osteosynthesis (external skeletal fixation, interlocking nail, bridging plate)
Decide whether to do Anatomic Reduction or Major Segment Alignment based on the following indications.
Indications for Anatomic Reconstruction or Major Segment Alignment
Anatomic Reconstruction
- Articular Fractures
- Single Fractures
- Fractures with one to three large fragments
Major Segment Alignment
Severely comminuted fractures treated with plates, plate/rod combination, interlocking nail, or external fixation.
Select the appropriate surgical approach (go to favorite textbook to select appropriate surgical approach) and make a surgical plan. (Go to the simulator) Determine if a cancellous bone autograft is needed and include it in your plan. Check your implant and instrument inventory re-evaluate your plans for reduction and fixation in light of the patient and the fracture, review the surgical approach, and precontour the plate if appropriate. Then perform the surgery.
After surgery critically inspect orthogonal radiographs of the operated bone which include the joint above and below the fracture to determine if the fixation accomplishes the mechanical goals of stabilizing the fracture then ask yourself if you preserved or added biological factors
To systematically evaluate postoperative radiographs, it is helpful to apply a mnemonic method of post operative radiographic evaluation such as the 4 A’s
- Alignment = Are the joints above and below aligned anatomically? If not, is the alignment acceptable (i.e. is the malalignment clinically relevant or is it mild)? If not acceptable, go back to the OR.
- Apposition/adjacency = Is there good fracture fragment apposition (if anatomical reconstruction was performed) or are the fragments within 2 bone diameters from the bone (if reconstruction was not attempted)?
- Apparatus = Evaluate your fixation – Is the size appropriate for the goals set forth? Are any screws in the joint, fracture, or physis? Are there open screw holes over the fracture site? Are the lengths of the screws/bolts/pins appropriate? Is the plate contoured appropriately?
- Activity = reserved for recheck radiographs to assess bone healing (Observe case 1, 6-week post op radiographs and then go to section on fracture healing)
Technical skills are developed with training programs, continuing education courses, and repetitive application of the surgical procedures.
Case Sample
Radiographs are made of the fractured bone (and frequently of the contra lateral bone to serve as a template for restoring limb alignment and bone length and as a guide to fixation size and contour). Fractures are classified according to the location of the fracture, (right or left, bone, location within the bone (diaphyseal, metaphyseal physeal, articular) and the direction and number of fracture lines. Along with learning to describe a fracture accurately to a specialist, much of the description gives you clues about the fracture to use in decision making and planning.
Transverse: perpendicular to the long axis of the bone
Oblique: runs at an angle to the long axis of the bone
- Short oblique = ≤ 45 degrees to the long axis
- Long oblique = ≥ 45 degrees to the long axis
– Spiral: wrap around the bone
– Comminuted: multiple fracture lines ( at least 3 pieces)
* Butterfly fragment = 2 oblique fracture lines with a large cortical fragment; (it is usually reducible)
*Highly comminuted = multiple pieces resembling a “shattered” appearance; ( usually non-reducible)
The displacement of the fracture on the current radiograph, the apparent reducibility of the fracture; and whether it is open to the environment.are all important descriptors
2-5 Come up with a fracture assessment score to guide your decision making for optimal treatment
After the patient has been thoroughly examined and life-threatening problems corrected, fracture treatment planning is performed. This includes assessing preoperative patient data such as age, weight, general health, activity level, and presence of other orthopedic pathology or neurologic pathology. Radiographs of the fractured and corresponding contralateral intact bones, which including the joints proximal and distal to the fracture; are closely examined as additional information can often be gathered (open physes are a dead giveaway that the patient is immature and biologically a healing machine and gas patterns at the fracture strongly suggest an open fracture. Client information such as their expectations and ability to perform postoperative care are also important to consider as you choose your fixation.
The mechanical score indicates how strong the implant must be.
A restored bone column which can transfer weight bearing load will help protect the implant from fatigue. Conversely an unreconstructed fracture depends on the implant to sustain the load of weight bearing. An animal with additional limb injuries or pre-existing pathology will be less able to protect the fractured limb and implant.
The Biological score indicates how long implant must function.
An immature animal with an active periosteum will heal very quickly. Conversely, an older or otherwise compromised animal will require a longer healing period. Fractures through the cancellous bone of the metaphysis will heal more quickly than diaphyseal fractures. Fractures with severely interrupted vascularity and disturbed surrounding soft tissues will require a longer healing period. Implants subjected to slow healing conditions must be larger, stronger and able to remain in position for extended periods to minimize chances for cyclic fatigue of the implant. Comminuted fractures with disturbed vascularity are best treated with biological techniques of major segment alignment and bridging osteosynthesis.
The clinical score indicates the level of postoperative care the owners can provide.
A co-operative animal with an attentive owner willing to follow directions is an asset. Active animals allowed excessive exercise must be treated with larger, stronger implants.
Come up with a FAS score from 1 to 10 by combining mechanical biological and clinical scores (see sample case for application of mechanical, biological and clinical assessment of the fracture and patient). Fractures with anticipated slow healing NEED functional implants for a long time. Implants subjected to unfavorable mechanical environments must be larger, stronger and remain in position for extended periods. An example would be adding ancillary fixation like an intramedullary pin (pin/plate combination), choosing a larger plate with more screws, or selecting an interlocking nail.
- 1-3 FAS tells you to use a very strong fixation and lots of biological as this animal may be a slow healer with inattentive owners
- A high middle score usually indicates an animal with a reconstructable fracture but unfavorable biology
- A low middle score may reflect a young dog with a severely comminuted fractur e which is nonreducible
- score of 8-10 indicates a healing machine with a reconstructable fracture and very attentive owners
Decide whether to perform an open or closed reduction by the following indications.
Review reduction videos
Open Reduction
- Articular Fractures
- Anatomically reconstructable fractures
- Comminuted fractures treated by major segment alignment and cancellous bone graft
Closed Reduction
- Nondisplaced or incomplete fractures
- Comminuted fractures treated by major segment alignment using bridging osteosynthesis (external skeletal fixation, interlocking nail, bridging plate)
Decide whether to do Anatomic Reduction or Major Segment Alignment based on the following indications.
Indications for Anatomic Reconstruction or Major Segment Alignment
Anatomic Reconstruction
- Articular Fractures
- Simple Fractures
- Fractures with one to three large fragments
Major Segment Alignment
Severely comminuted fractures treated with plates, plate/rod combination, interlocking nail, or external fixation.
Select the appropriate surgical approach (go to favorite textbook to select appropriate surgical approach) and make a surgical plan. (Go to the simulator) Determine if a cancellous bone autograft is needed and include it in your plan. Check your implant and instrument inventory re-evaluate your plans for reduction and fixation in light of the patient and the fracture, review the surgical approach, and precontour the plate if appropriate. Then perform the surgery.
After surgery critically inspect orthogonal radiographs of the operated bone which include the joint above and below the fracture to determine if the fixation accomplishes the mechanical goals of stabilizing the fracture then ask yourself if you preserved or added biological factors
To systematically evaluate postoperative radiographs, it is helpful to apply a mnemonic method of post operative radiographic evaluation such as the 4 A’s
- Alignment = Are the joints above and below aligned anatomically? If not, is the alignment acceptable (i.e. is the malalignment clinically relevant or is it mild)? If not acceptable, go back to the OR.
- Apposition/adjacency = Is there good fracture fragment apposition (if anatomical reconstruction was performed) or are the fragments within 2 bone diameters from the bone (if reconstruction was not attempted)?
- Apparatus = Evaluate your fixation – Is the size appropriate for the goals set forth? Are any screws in the joint, fracture, or physis? Are there open screw holes over the fracture site? Are the lengths of the screws/bolts/pins appropriate? Is the plate contoured appropriately?
- Activity = reserved for recheck radiographs to assess bone healing (Go to fracture healing)
Technical skills are developed with training programs, continuing education courses, and repetitive application of the surgical procedures.