
Healing Overview:
Fracture healing is modulated by the biological and mechanical environment of the fracture. The biological environment of the fracture determines the speed of bone healing. Provided there is adequate vascularity, the mechanical environment or stability at the fracture determines the pattern of bone healing which can range from direct bone formation to indirect bone union via endochondral ossification.
Clinical Union is by definition when a fracture has healed sufficiently to safely remove the support without the risk of refracture. Understanding the cellular process occurring with different patterns of bone healing and using that understanding to interpret the corresponding radiographic images is essential for accurate post-operative care. As long as the fracture is not bridged with bone, exercise is controlled and the fixation left in place or, in the case of external fixators, destabilized to promote bone formation. Casts or implants allowing callus formation usually have to be removed by 6 weeks which is why they are reserved for rapidly healing fractures
Strain
Definition and Impact:
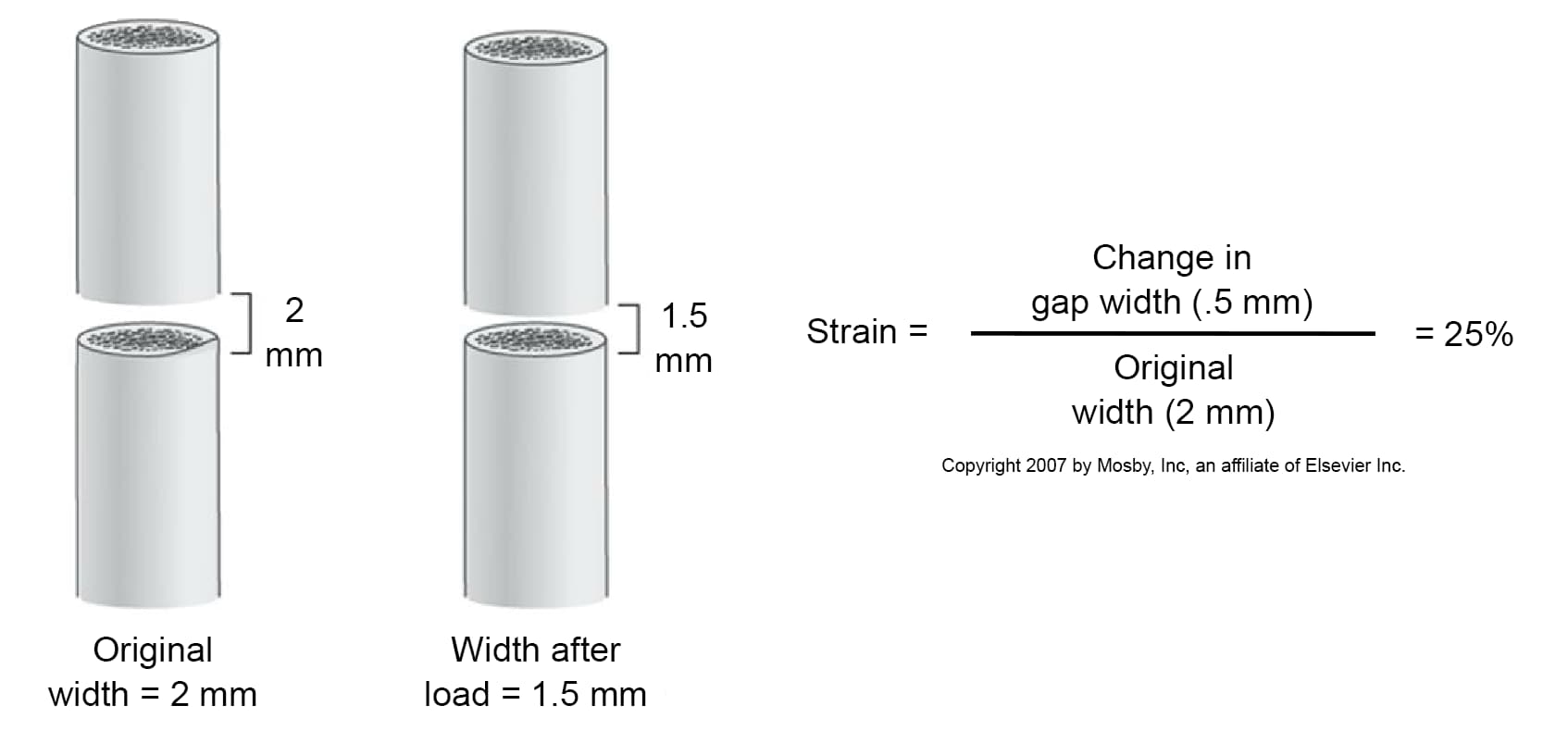
Motion at the fracture is described by the concept of strain. Strain is calculated by dividing the original width of the fracture by the change in width occurring with motion and is expressed as a percent. The strain environment dictates the type of tissue formed at the fracture. Granulation tissue can form in 100% strain environments. Connective tissue forms in a strain environment of 20%. Fibrocartilage can form in a strain environment of 10%. Bone can only form in a strain environment of 2% or less.
Fragment Effect on Strain:
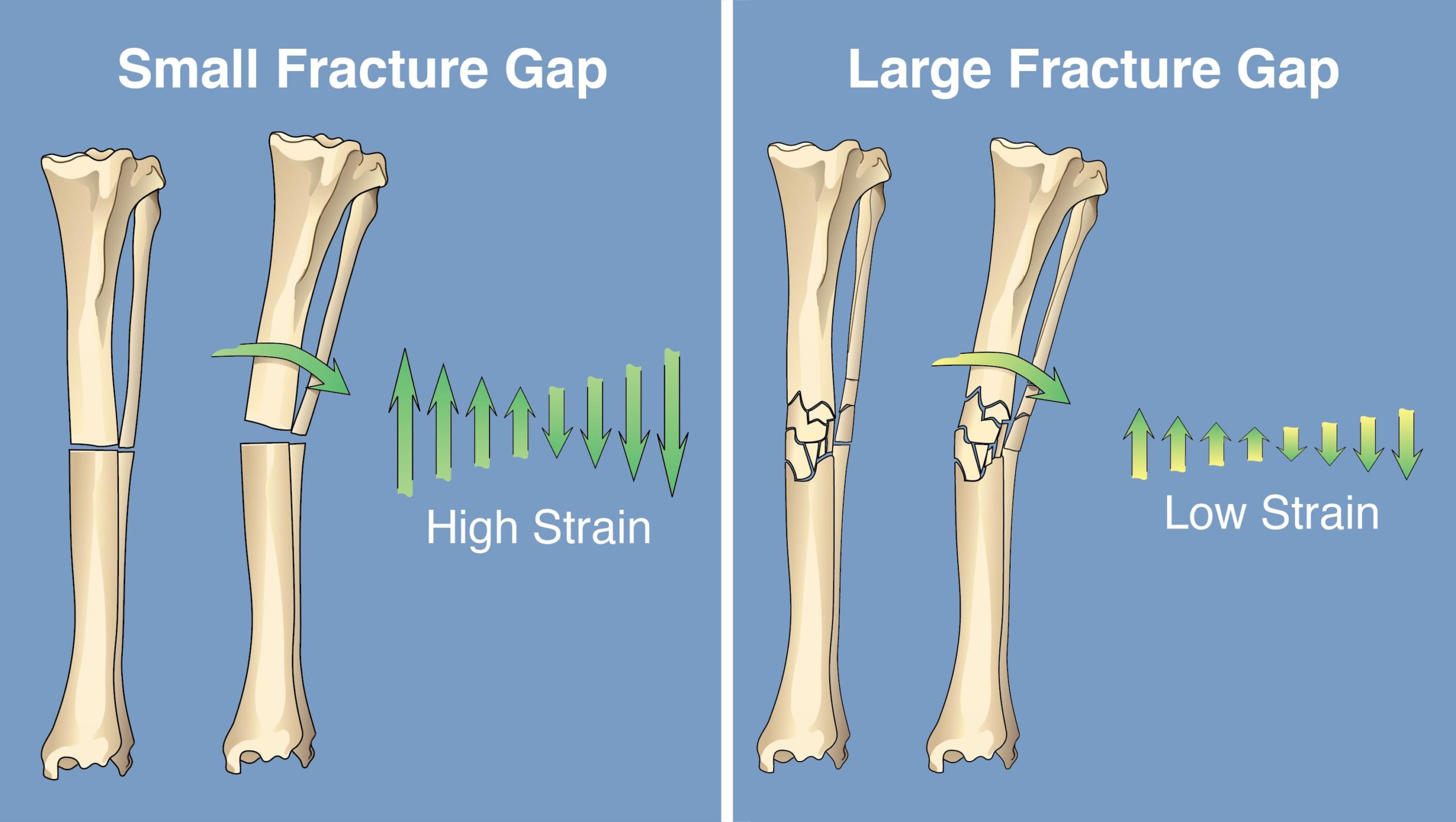
Multifragment fractures distribute strain across the fracture area, decreasing the strain environment in comparison to single fractures.
Nature’s Way to Minimize Strain:
The strain environment is decreased by natural healing processes found in indirect bone healing such as bone resorption at the fracture which widens the original width of the fracture; endochondral ossification where tissues are formed in an orderly pattern according to the strain environment; and periosteal callus formation which increases the diameter of the bone at the fracture site thereby greatly increasing the ability of the bone to resist bending and torsional forces.
Operative Treatment to Minimize Strain:
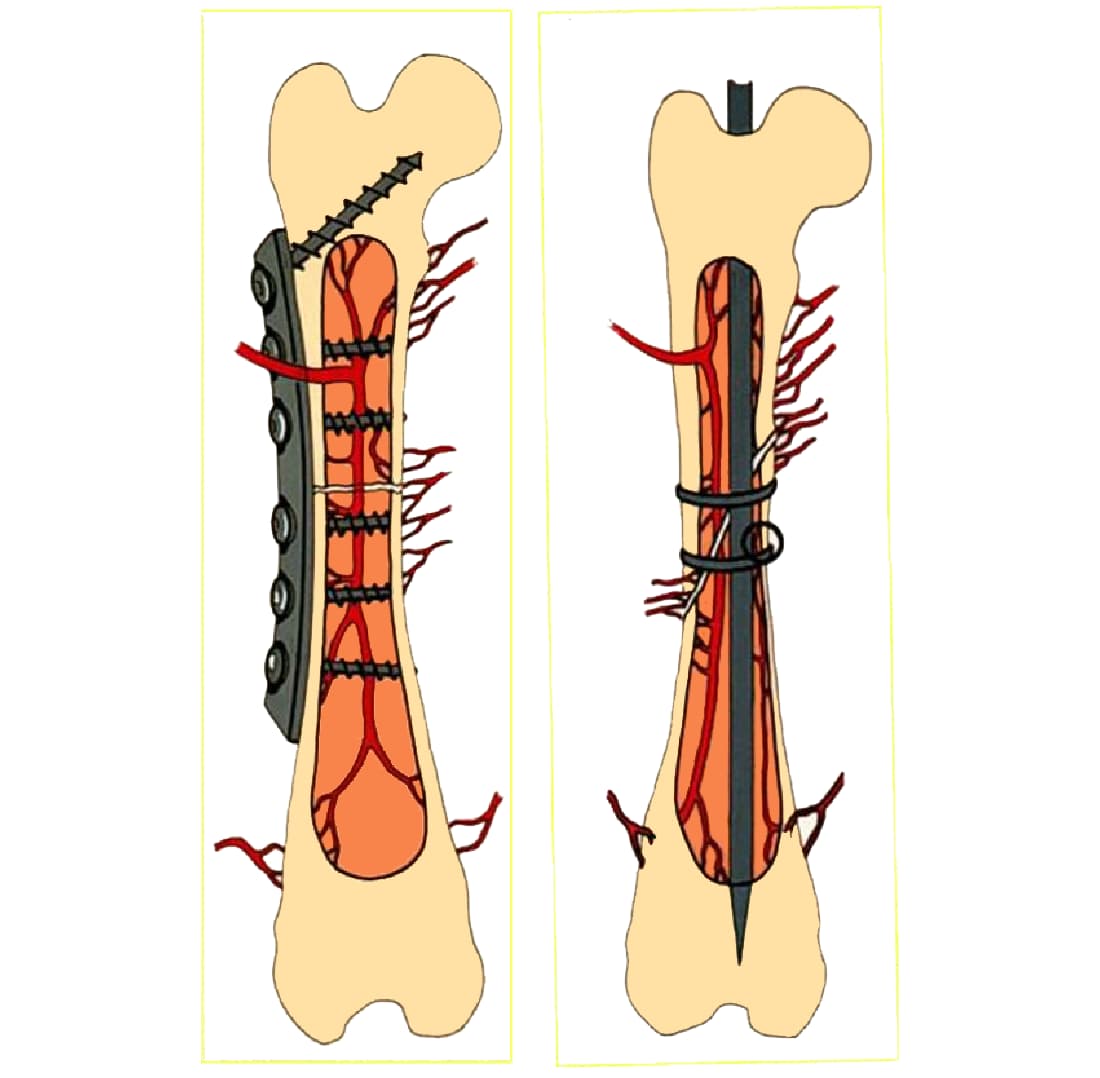
The strain environment is greatly affected by the operative treatment of the fracture. Compression of the fracture with plate or lag screw application results in a very low strain environment. Strain increases with the increasing motion associated with various types of external fixator frames, interlocking nails, and cast application respectively.


Indirect Bone Healing:
Indirect bone healing occurs in fractures with a more compliant fixation. Allowing motion at the fracture.
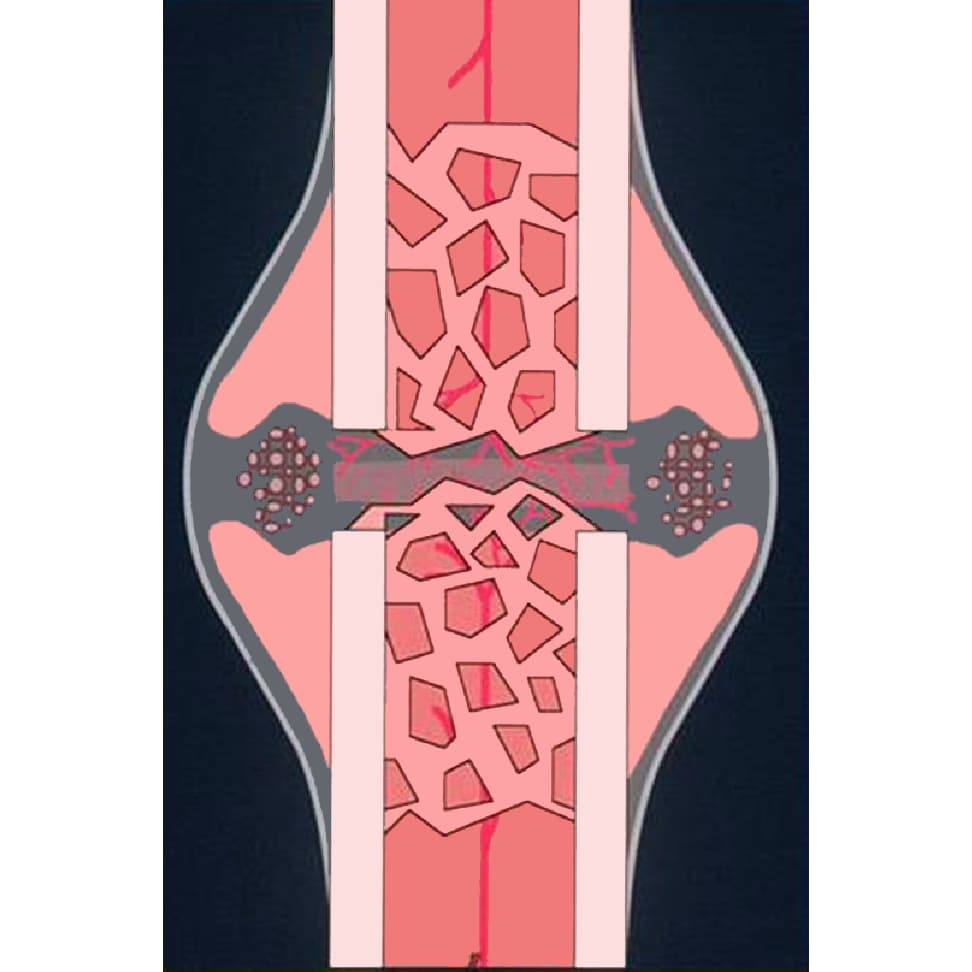
Press button 1. Remember that the extraosseous blood supply (red vessels extending into the fracture and the growth factors found in the fracture hematoma are paramount for healing. Granulation tissue (blue) which survives in strains up to 100% infiltrates the fracture site first (note the movement at the fracture). This tissue slightly stabilizes the fracture to allow the gradual formation of connective tissue and fibrocartilage (orange) which survive in strains of 20 and 10% respectively, and in turn continue to stabilize the fracture site.
Press button 2. Bone callus (bone-colored chips) forms first on the relatively stable endosteal and periosteal bone surfaces. These processes continue until the strain environment is less than 2% and mineralization of the fibrocartilage (purple) occurs beginning at the fragment surfaces and moving toward the center of the gap.
Press button 3. Local resorption of the mineralized tissue is followed by the formation of bridging bone callus.
Press button 4. Continued formation and resorption of bone at the fracture site results in remodeling of the callus to cortical bone.
Press button 5. Implants (or casts) are removed when bone bridges the fractures on all radiographic views.
Direct Bone Healing:
Direct bone healing occurs when there is rigid fixation of the fragments with contact or very small (200-500 microns) gaps between bone ends resulting in a gap strain of less than 2%.
Press button 1. Where there are small gaps between bone ends (press the button labeled gap) a randomly oriented network of fibrous bone is first deposited within the gap, (pink wavy chips) followed by osteonal remodeling (Press the pink remodeling unit to see its makeup of osteoclasts cutting through the bone followed by osteoblasts laying down osteoid which is turned into the bone of an osteon all nourished by a blood vessel. Press it again to close the view. Ostonal remodeling begins as early as the third week after fracture and intensifies during the fifth and sixth weeks after fracture. Now press the button labeled contact. When a fracture is compressed by a plate or a bone screw placed as a lag screw some areas of the fracture are in contact. Here osteonal remodeling is the sole step in bone healing. Press the back button.
Press button 2. Once again look at the gap and the contact areas. The progress of each remodeling unit is about 70-100 microns per day. This process slowly unites the bone fragments with lamellar bone structures arranged parallel to the long axis of the bone through the fragment ends and across the fracture gap. Think of it as healing by the placement of dowel rods across the fracture.
Press button 3. Examine the bone formation in the areas of contact and gap (left and right cortices). In direct bone healing the plate acts as the callus and is usually left in place for 5 to 14 months after union of the fragments.
Intramembranous Bone Healing:
Comminuted fractures fixed with biological techniques of indirect reduction, major segment alignment and optimal stabilization appear to heal with an intramembranous type of bone formation.
Press button 1. This is a combination of direct differentiation of mesynchymal cells to osteoblasts and endochondral ossification within the fracture hematoma.
Press button 2. There is minimal periosteal callus formation with the endosteal and bridging callus supplying most of the fracture repair.
Press button 3. Resorption of woven bone and formation of lamellar bone at the fracture sites result in remodeling of bony callus to cortical bone This can be encouraged by destabilizing the fixation to allow more forces directed through the fracture.
Press button 4. All implants can be removed when bone bridges the fractures on all radiographic views.
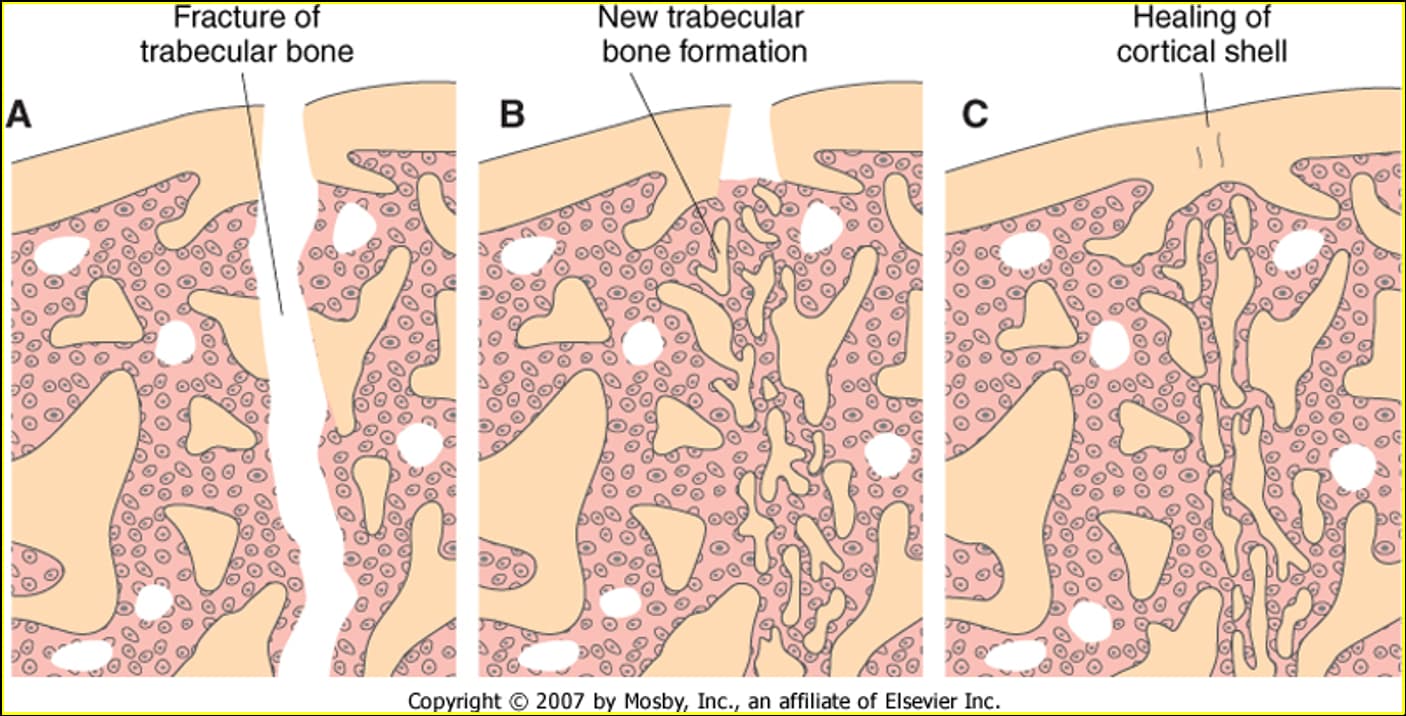
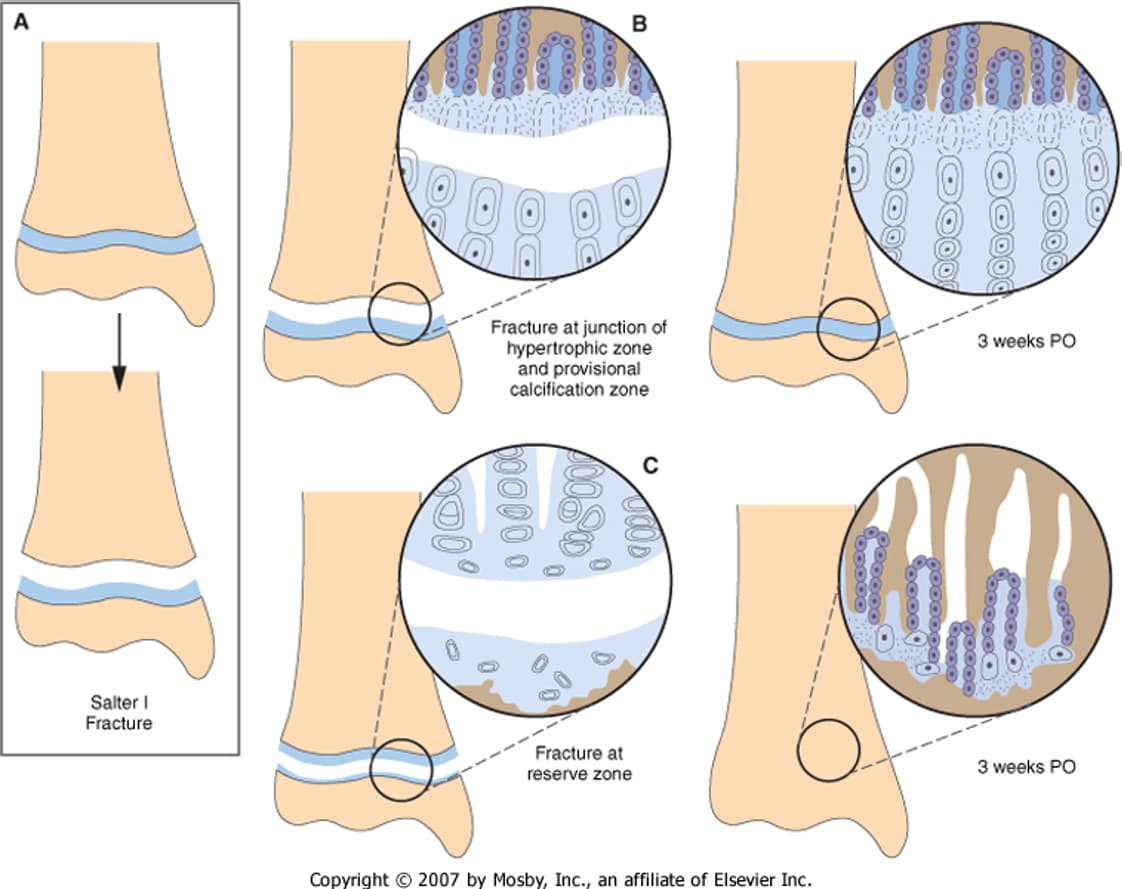
Metaphyseal Bone Healing and Physeal Healing:
See lectures and references
Metaphyseal Bone Healing
Physeal Bone Healing
Delayed Unions and Non-Unions:
(see lectures and references)
Delayed Union is defined-as a longer than normal fracture healing time. Causes may be undeterminable. Serial radiographs are made to document slowly progressive healing. As long as implants are stable the bone should eventually heal. A cancellous bone graft may be helpful.
Non-Unions: Fractures that fail to heal without surgical intervention. The most common nonunions are caused by inadequate stabilization and have hypertrophic callus formation at the fracture. Treatment consists of surgical stabilization with compression of the fracture. Autogenous bone graft, bone marrow, or other growth factors (bmp-2, bmp-7) may be useful. in many fractures the callus can supply cancellous bone