
ESSENTIAL TRAINING
Fracture Management
INTRODUCTION
- Orthopedic examination, localization of the problem, and differential diagnoses. The decision making is focused on identifying the problem.
- It also includes neurological examination and localization of diseases affecting the spine again focusing on identifying the problem.
- Finally it includes fracture management with the decision making focused on the treatment
- Orthopedic differential diagnosis developed during orthopedic examination with “limping Louis”
- Orthopedic maneuvers performed during physical examination to determine abnormality. ( ie drawer sign, ortoloni )
- Biology of selected orthopedic diseases (hip dysplasia, OCD)
- Identify spinal lesion location during neurological examination with “spinal Sally lesion locater (SSLL)
- Fracture treatment planning including the fracture treatment simulator and
- Fracture reduction techniques
- Biology of diaphyseal healing including direct: indirect: intramembranous bone healing
- Case management: design so teacher can easily plug in case: including animal picture; preop rads fx(s) ,chest, abdomen, miscellaneous; po and follow up rads
- Worksheet for learners
Fracture Planning:
Developing an appropriate plan involves the following interrelated steps.
1. Gather information about the fracture, patient, client and environment for the animal and make a decision regarding appropriate types of fixation.
2. Make a detailed plan for achieving fracture reduction. Decide whether to perform an open or closed reduction.
Indications for Open or Closed Reduction
Open Reduction
Articular Fractures
Anatomically reconstructable fractures
Comminuted fractures treated by major segment alignment and cancellous bone graft
Closed Reduction
Nondisplaced or incomplete fractures
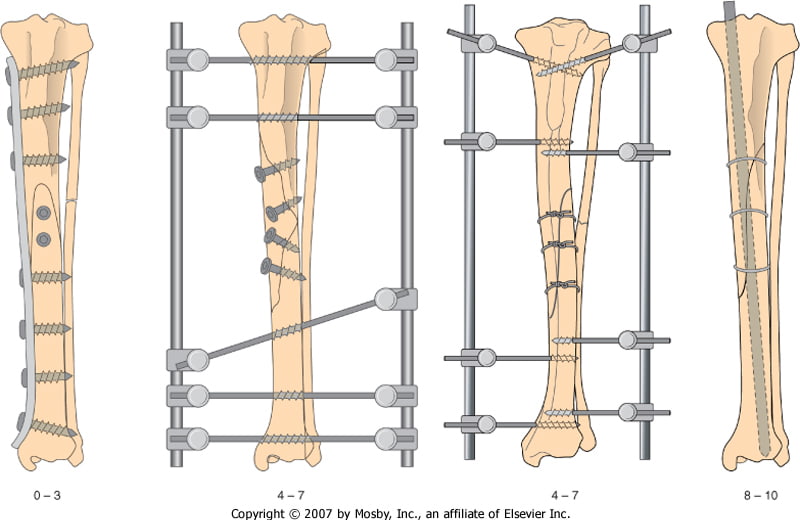
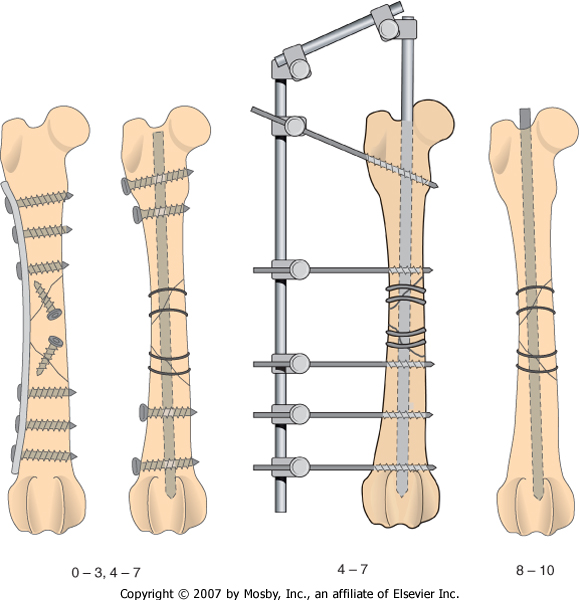
Comminuted fractures treated by major segment alignment using bridging osteosynthesis (external skeletal fixation, interlocking nail, bridging plate)
3. Make a detailed plan for either Anatomic Reduction or Major Segment Alignment.
Indications for Anatomic Reconstruction or Major Segment Alignment
Anatomic Reconstruction
-Articular Fractures
-Simple Fractures
Fractures with one to three large fragments
Major Segment Alignment
Severely comminuted fractures treated wit plates, plate/rod combination, interlocking nail, or external fixation
- Select the appropriate surgical approach (go to favorite textbook to select appropriate surgical approach), and make
a surgical plan. Determine if a cancellous bone autograft is needed and include it in your plan.
- Check your implant and instrument inventory,
re-evaluate your plans for reduction and fixation in light of the patient and the fracture, review the surgical approach, and precontour the plate if appropriate.
- Perform the surgery.
- Critically evaluate your postoperative radiographs to determine if you met your goals.
Use the 4 A’s
Use the 4 A’s:
– Alignment = Are the joints above and below aligned anatomically? If not, is the alignment acceptable (i.e. is the malalignment clinically relevant or is it mild)? If not acceptable, go back to the OR.
– Apposition/adjacency = Is there good fracture fragment apposition (if anatomical reconstruction was performed) or are the fragments within 2 bone diameters from the bone (if reconstruction was not attempted)?
– Apparatus = Evaluate your fixation – Is the size appropriate for the goals set forth? Are any screws in the joint, fracture, or physis? Are there open screw holes over the fracture site? Are the lengths of the screws/bolts/pins appropriate? Is the plate contoured appropriately?
– Activity = reserved for recheck radiographs to assess bone healing
Technical skills are developed with training programs, continuing education courses, and repetitive application of the surgical procedures.

Procedure Overview:
The objectives in treating fractures, non-unions or bone deformities are bone union and the patient’s return to normal function. Appropriate decision-making processes to choose the implants, thorough planning of the procedure, and using good technical skills to apply the implants should produce consistent and predictable results. There are many different methods for providing fracture stability. The decision-making process helps the surgeon to identify which implants will achieve the necessary stability for the appropriate time to satisfy the objectives. It is also important to make a detailed plan for the entire surgical operation. Failure to plan the procedure results in prolonged operating times, excessive soft tissue trauma and technical errors. The outcomes of improper planning are implant failure, delayed healing, infection, and non-union. Although it is easy for the busy veterinary surgeon to be pressured into performing surgery after a cursory examination of the radiographs, failure to adequately plan the procedure will result in erratic outcomes.
Fracture Classification:
Radiographs must be made of the fractured bone (and frequently of the contra lateral bone to serve as a template for restoring limb alignment and bone length and as a guide to fixation size and contour).
Long bone fractures are classified according to the location, direction and number of fracture lines; the reducibility of the fracture; and whether they are open to the environment.
For fracture fixation planning, fractures should be classified as anatomically reconstructable or non-reconstructable (those with multiple small pieces).
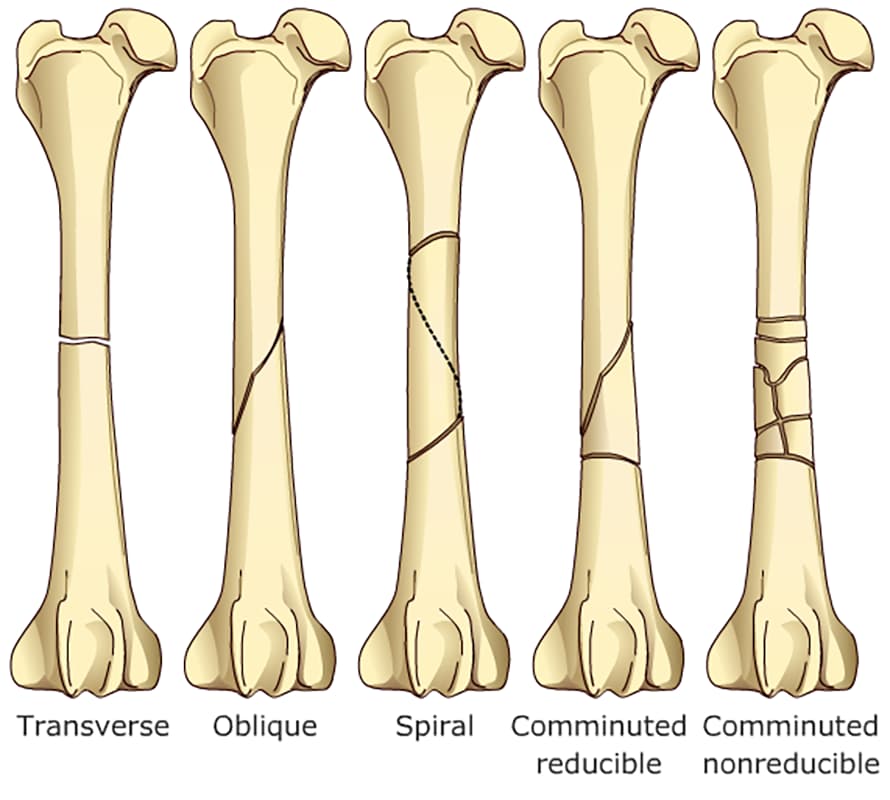
Types of fractures:
– Transverse: perpendicular to the long axis of the bone
– Oblique: runs at an angle to the long axis of the bone
* Short oblique = ≤ 45 degrees to the long axis
* Long oblique = ≥ 45 degrees to the long axis
– Spiral: wrap around the bone
– Comminuted: multiple fracture lines in at least 3 pieces
* Butterfly fragment = 2 oblique fracture lines with a large cortical fragment; reconstructable
*Highly comminuted = multiple pieces resembling a “shattered” appearance; non-reconstructable
Decision Making:
After the patient has been thoroughly examined and life-threatening problems corrected, preoperative fracture planning is performed. The most important part of fracture planning is gathering preoperative data to determine a mechanical, biological and clinical assessment of the fracture and patient. Preoperative data includes patient information such as age, weight, general health, activity level, and presence of other orthopedic pathology or neurologic pathology; radiographs of the fractured and corresponding contralateral intact bones, which include the joints proximal and distal to the fracture; and client information such as their expectations and ability to perform postoperative care. This data establishes the mechanical, biological, and clinical environment in which the implants must function.
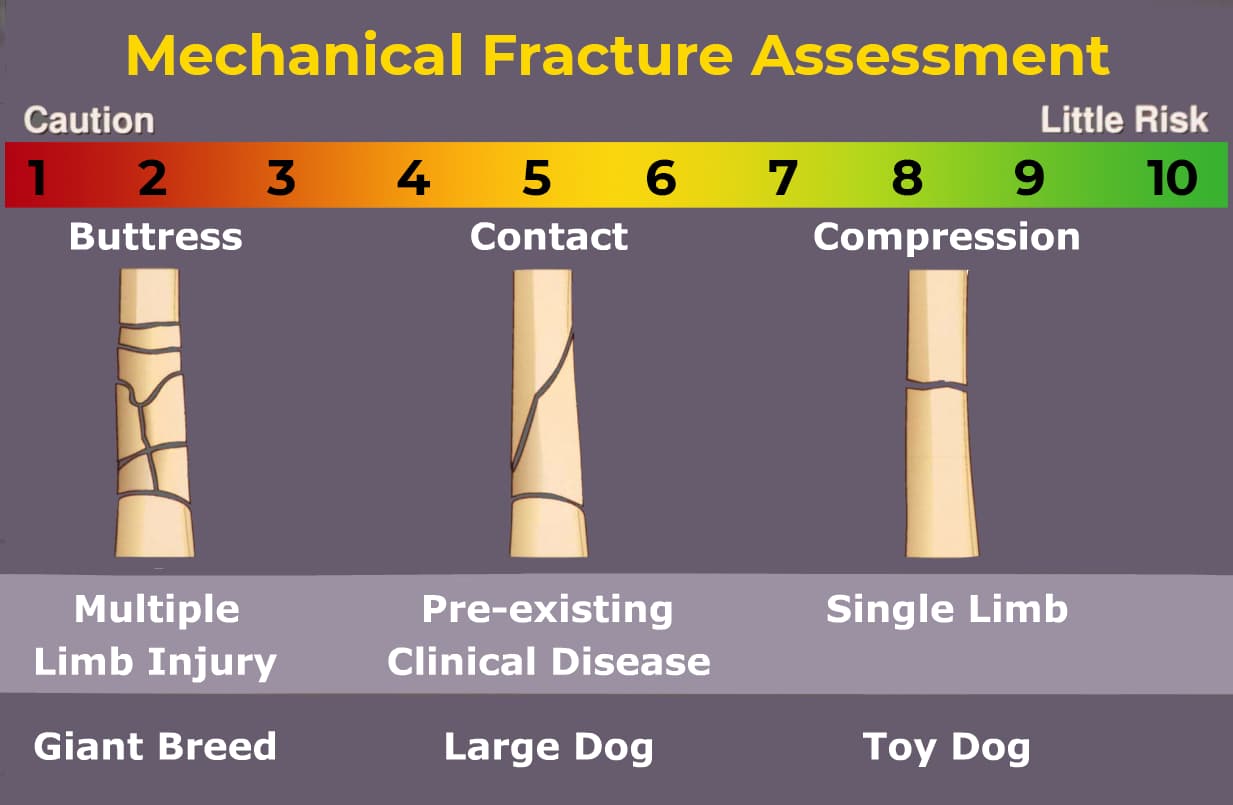
Mechanical Environment:
A restored bone column which can transfer weight bearing load will help protect the implant from fatigue. Conversely an unreconstructed fracture depends on the implant to sustain the load of weight bearing. An animal with additional limb injuries or pre-existing pathology will be less able to protect the fractured limb and implant. Fractures with anticipated slow healing (older animals or comminuted fractures with soft tissue loss) need functional implants for a long time. Implants subjected to unfavorable mechanical environments must be larger, stronger and remain in position for extended periods. An example would be adding ancillary fixation like an intramedullary pin (pin/plate combination), choosing a larger plate with more screws, or selecting an interlocking nail.
Mechanical score indicates how strong implant must be.
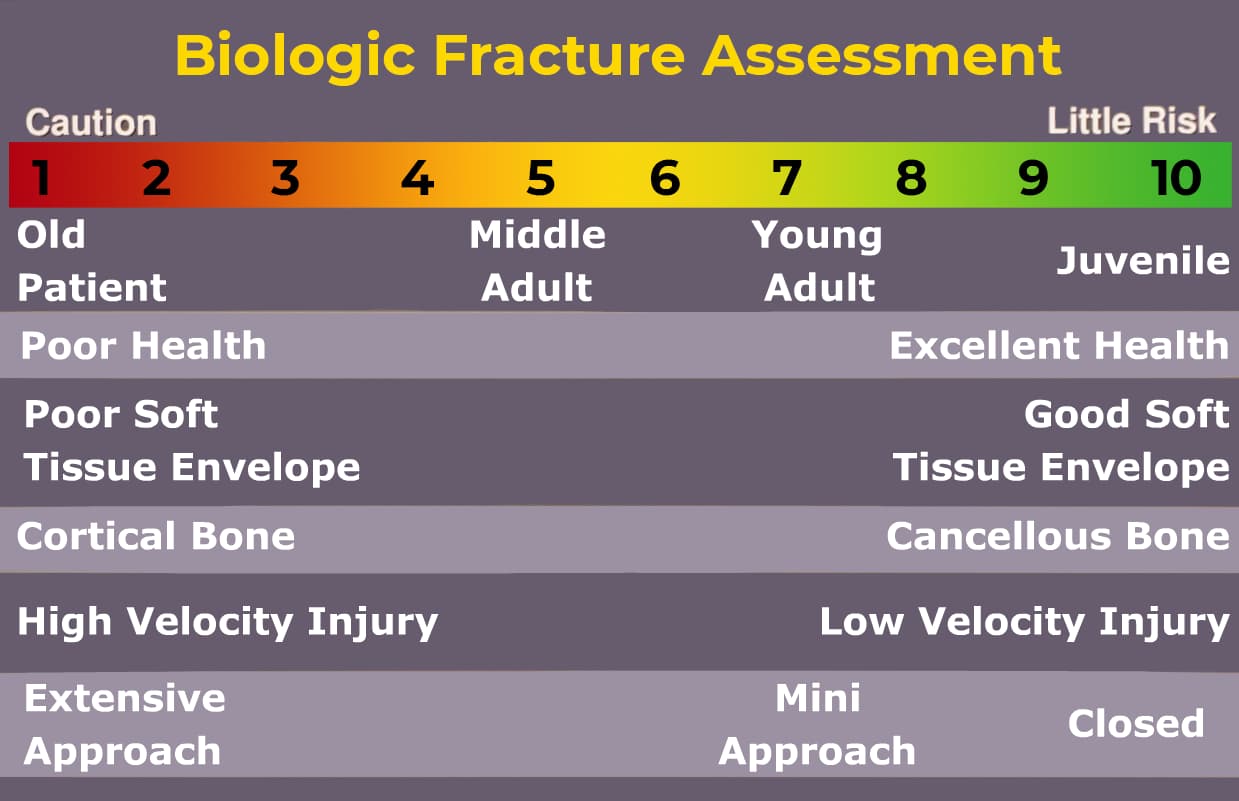
Biological Environment:
An immature animal with an active periosteum will heal very quickly. Conversely, an older or otherwise compromised animal will require a longer healing period. Fractures through the cancellous bone of the metaphysis will heal more quickly than diaphyseal fractures. Fractures with severely interrupted vascularity and disturbed surrounding soft tissues will require a longer healing period. Implants subjected to slow healing conditions must be larger, stronger and able to remain in position for extended periods to minimize chances for cyclic fatigue of the implant. Comminuted fractures with disturbed vascularity are best treated with biological techniques of major segment alignment and bridging osteosynthesis methods.
Biological score indicates how long implant must function.
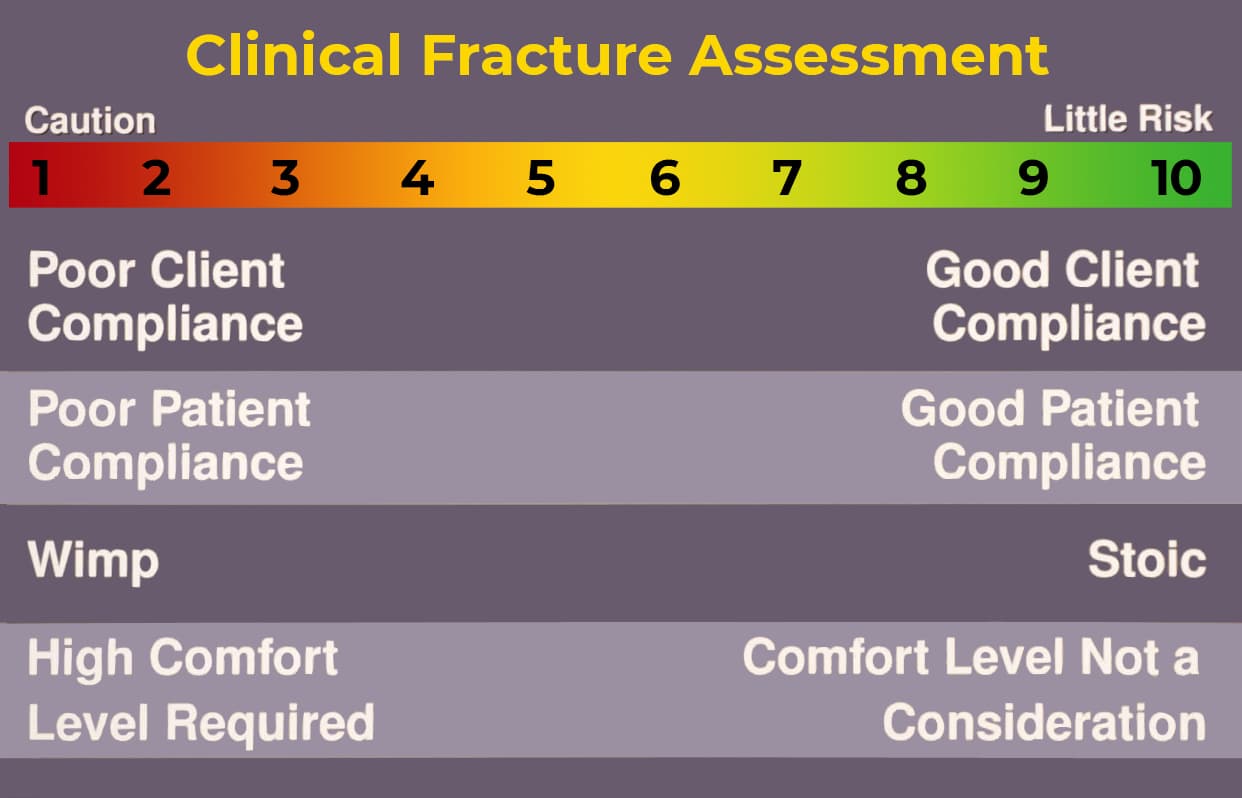
Clinical Environment:
A co-operative animal with an attentive owner willing to follow directions is an asset. Active animals allowed excessive exercise must be treated with larger, stronger implants.