
Dr. Jenica Haraschak is a clinical assistant professor in the small animal emergency and critical care service.
Fluid therapy is one of the most common therapies prescribed in veterinary medicine. To create a fluid therapy plan, the clinician must have a basic understanding of body fluid compartments, composition of available fluids, components used to formulate a fluid therapy plan, and possible complications.
In dogs and cats, total body water (TBW) is 60% of ideal body weight (BW) and represents the sum of intracellular and extracellular fluid volumes. TBW is divided into intracellular (40% of TBW) and extracellular (20% of TBW) compartments. The extracellular compartment is further divided into the interstitial (12% to 15% of TBW) and intravascular (6% to 8% of TBW) spaces. Loss of fluid in the intravascular space leads to hypovolemia, whereas loss of fluid from the interstitial or intracellular spaces leads to dehydration.
Fluids can be divided into three categories based on their composition. Isotonic crystalloids (0.9% NaCl, LRS, Normosol-R) have an osmolality and electrolyte composition similar to plasma. LRS and Normosol-R are additionally considered balanced solutions because they contain a buffer, which helps to maintain or normalize acid-base disturbances. Hypotonic crystalloids (0.45% NaCl) have a lower electrolyte composition, whereas hypertonic crystalloids (7.2% NaCl) have a higher electrolyte composition compared to plasma, and therefore both will cause water to shift between body compartments.
Route of Fluid Administration
Multiple routes for fluid administration exist. Subcutaneous (SQ) fluids should be used to treat patients with mild dehydration or to maintain daily fluid requirements, such as in patients with chronic kidney disease. Doses for SQ fluids range from 10 to 30 ml/kg. The volume should not exceed 20 ml/kg per injection site. SQ fluids should be a balanced isotonic crystalloid without any additives (dextrose or potassium chloride), which can cause local tissue damage and patient discomfort.
Intravenous fluids (IV) are indicated for rapid and more accurate administration of fluid volumes. They are used to treat hypovolemia, moderate to severe dehydration, and electrolyte and acid-base disturbances and to provide daily maintenance fluid requirements.
Enteral water is a commonly forgotten route for fluid administration but can be very effective for correcting mild dehydration or providing maintenance fluid requirements. Patients that are not voluntarily eating or drinking may require placement of an indwelling feeding tube (nasogastric or nasoesophageal). Similar maintenance fluid rates can be used for enteral water, and the total volume can be given as a 24-hour CRI or divided into smaller volumes, given every 4 to 6 hours. Patients with prolonged anorexia should be started at a lower volume and gradually increased to reduce the risk of intolerance.
Phases of Fluid Therapy
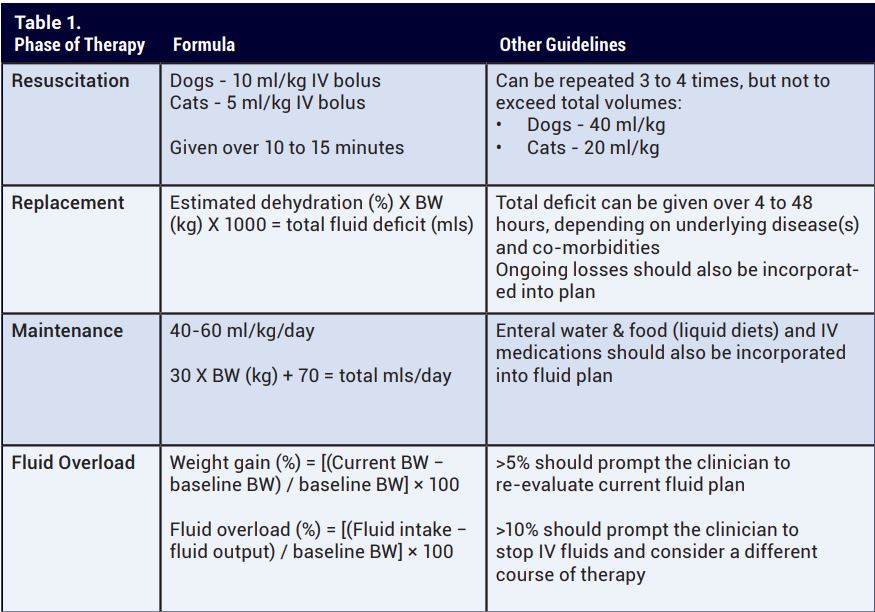
During the resuscitation or stabilization phase, IV fluids are used to correct acute intravascular fluid deficits associated with hypovolemia and hypoperfusion. Intravenous volume is based on total circulating blood volume, which is 80 to 90 ml/kg in dogs and 50 to 60 ml/kg in cats. Historically fluid boluses were given in volumes equal to 1/4 of the blood volume (22 ml/kg for dogs; 15 ml/kg for cats). Newer guidelines, however, recommend smaller volumes (10 ml/kg for dogs; 5 ml/ kg for cats).
Fluid boluses should be administered rapidly (within 10 to 15 minutes) with serial assessment of perfusion parameters, including mentation, heart rate, pulse quality, mucous membrane color, capillary refill time, blood pressure, and lactate. If ongoing signs of hypoperfusion exist, additional therapies, such as colloids or vasopressors, should be considered. Clinically, there is no disease process or medical condition in which the entire blood volume should be replaced using crystalloid fluids. In patients with severe hemorrhage, blood products are the preferred resuscitation fluid.
The replacement or rehydration phase is determined based on hydration status and ongoing losses. In any disease process, acute fluid loss originates from the intravascular space, which causes water and electrolytes to shift from the interstitial and intracellular compartments.
Dehydration is a very subjective assessment that is determined based on patient parameters including skin turgor, mucous membrane moisture, corneal moisture, and eye position. The patient’s age and body condition may lead to an inaccurate assessment of hydration status. Geriatric and cachectic animals have less skin elasticity, whereas puppies and kittens have increased skin elasticity. Mucous membrane moisture is the most inaccurate parameter to assess because panting, a dry environment (oxygen cage), or nausea/excessive drool can lead to an inaccurate assessment by the clinician.
Estimated dehydration deficits can be replaced over a wide range (4 hours to 48 hours) depending on the patient’s underlying disease(s) and co-morbidities. It’s important to remember that dehydration is only an estimate and highlights the importance of reassessing the patient’s hydration status at least once daily and adjusting the fluid plan as indicated. Monitoring body weight is the most sensitive and readily available method to assess changes in body water and hydration status. Patients should be weighed at least once daily or multiple times a day if they have excessive ongoing losses (vomiting, diarrhea, polyuria, etc.), kidney disease, heart disease, or are at risk for fluid overload.
A fluid therapy plan requires the clinician to accurately assess fluid deficits, identify and treat the underlying cause of fluid and electrolyte loss, create a fluid plan that meets the specific needs of the patient, and monitor the response to fluid therapy.
Maintenance fluid therapy plans are designed to provide water and electrolytes in quantities that meet the normal daily fluid requirements, in addition to replacing urinary, gastrointestinal, and evaporative losses. Many formulas exist to determine the maintenance fluid requirements (See Table 1). Either hypotonic or isotonic fluids can fulfill maintenance requirements, although prolonged use of isotonic fluids can result in iatrogenic hypernatremia and hyperchloremia due to the higher sodium and chloride concentrations. Clinicians should also keep in mind all sources of fluids when determining a fluid plan, including commonly overlooked sources such as IV medications and food/water.
Complications of Fluid Therapy
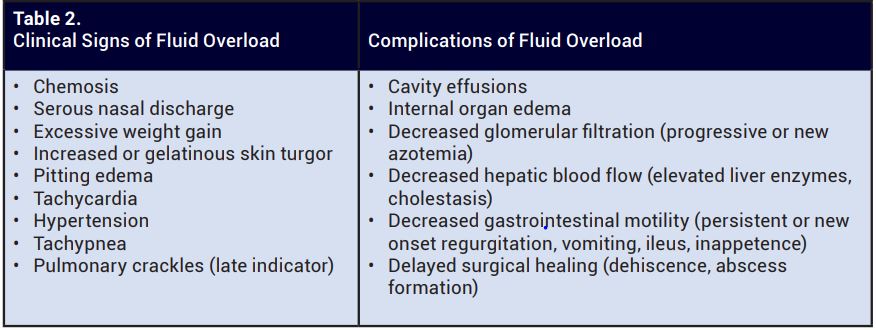
Fluid overload is defined as a pathologic accumulation of extravascular body water secondary to excessive fluid administration and has been associated with increased patient morbidity and mortality. Fluid overload occurs most commonly secondary to overzealous fluid therapy or failure to correlate a fluid plan with fluid requirements.
Additionally, the risk of fluid overload rises in certain disease states: severe systemic inflammation (pancreatitis, sepsis, trauma, surgery, etc.), hypoproteinemia, kidney disease, and cardiac disease. Feline patients are less tolerant of aggressive fluid rates due to their smaller blood volume, lower metabolic rate, and occult heart disease. They are at a higher risk of complications associated with an inappropriate fluid plan.
Note to Referrers:
The Small Animal Emergency Service is currently unable to provide outpatient or same-day imaging services (ultrasound, CT scan). Nor can we guarantee consultations or hospitalization/transfer to another specialty service.
To provide excellent service to both you and your clients, we request that you call before referring your patient to the ER so we can provide appropriate expectations and cost estimates in advance.
For patients not requiring emergency care, clients may be asked to schedule an appointment with one of our specialty services. The Emergency and Critical Care Service is available 24/7 for phone consultations and to assist with case management. If you have any questions, please do not hesitate to contact us: 217-333-5311.


